

double flap design envelope video
Open access peer-reviewed chapter
Flap Techniques in Dentoalveolar Surgery
By Randa Abdulmoein AlFotawi
Submitted: June 20th 2019 Reviewed: January 13th 2020 Published: May 13th 2020
DOI: 10.5772/intechopen.91165
Abstract
Most dentoalveolar procedures involve the reflection of mucosal flaps. This step is crucial for exposure or removal of impacted teeth, implant bed preparation, exposure of the alveolar bone for augmentation, periodontal surgeries, and repair of mucosal soft tissue defects, such as oroantral fistula. Because of the rich vascularity of the oral mucosa, great freedom is allowed for flap design, but it tends to result in carelessness and lack of thoughtful planning, which may lead to uneventful outcomes or/and complications. In this chapter, we review oral anatomy, classification, indications, and complications of common oral flap techniques; common flap designs are illustrated, and their fundamental principles are highlighted. The review has covered various flap designs based on their indications. Yet the common flap's principles are fundamental for all types of flaps regardless of their application, namely, it should provide wide exposure, clear vision, good access, and assure rich vascularity and good final aesthetic outcome.
Keywords
- flap principle
- applications
- classification
- flap technique
1. Introduction
Oral surgical flap by definition is the operation in which a portion of the mucoperiosteal tissue is surgically detached from the underlying bone for better access and visibility. Common principles have been applied for all flap designs. First, the base of the flap should be broader than the free end to ensure adequate blood supply. Second, the incision should be performed at a right angle to the underlying bone, avoiding any anatomical structures, and it should provide adequate visualization. Third, the flap should be wider than the anticipated underlying bone defect and delicately handled without tension. Fourth, the vertical releasing incision should start from the buccal vestibule and end up mesial or distal to the interdental papilla. Different flaps have been proposed for various intraoral surgeries, that is, third molar surgery, canine exposure, various periodontal surgery, dental implant preparation, endodontic surgeries, and repair of oroantrual communications. The review will focus on oral anatomy, classification, indications, complications of common oral flap techniques; common flap designs are illustrated, and their fundamental principles are highlighted.
Advertisement
2. Third molar surgery
2.1 Background
The flap design has considerable effects on primary wound healing in lower third molar surgery [1]. When the conventional sulcular flap design is used, 56% of the patients develop a disorder in primary wound healing [1]. The envelope flap is fixed anteriorly with intersulcular sutures. Notably, dehiscence can take place inconspicuously and unnoticed by the patient and may heal secondarily. The secondary wound healing can cause wedge-shaped defects of the gingiva distal to the second molar or can lead to a loss of attachment distal to the second molar. This periodontal complication after lower third molar surgery has been investigated by several studies [2, 3, 4, 5]. Dehiscence occurs in only 10% of cases of triangular flap design [1], and the triangular flap design decreases tension in the area distal to wound closure compared with the envelope flap technique. The vestibular triangular flap can be easily moved to the lingual, ensuring a wound closure that is almost tension-free. The mesial vestibular relieving incision, which is only adapted coronally by a single suture, allows depletion of the postoperative hematoma during masticatory movements. On the first postoperative day, a present hematoma is easy to relieve by spreading and compression. The advantage is that the release area has bone support. Such postoperative morbidity has important medical-legal and economic implications. Many surgical approaches, such as those with the use of surgical drains, different wound closure techniques, and various flap designs, have been tried to minimize the complications [6].
2.2 Envelope flap
An envelope flap with a sulcular incision from the first to the second molar and a distal relieving incision to the mandibular ramus is a widely used technique for lower third molar surgery (Figure 1).
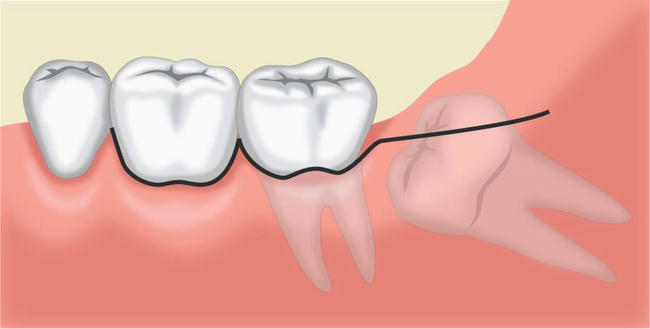
Figure 1.
Envelope flap for the removal of the third molar.
The envelope flap is closed with two or three single button sutures distal to the second molar, with special attention to an exact repositioning in the area of the gingival margin. In addition, the flap is adapted with interdental sutures between the first and the second molars.
Advantages
-
Good exposure during surgery
-
Mesial cut could be extended if cystic surgery or endosurgery is required
-
The envelope flap provides adequate soft tissues, covering for any bone defects
-
The envelope flap has a wider base, assuring vascularity up to the wound margins
Limitations
-
Inducing loss of the alveolar bone distal to the second molar probably due to wound dehiscence
-
Sulcular incision may lead to periodontal damage
-
The envelope flap leads to a total loss of the attached gingiva in this area after the operation, thus causing pocket formation and loss of attachment in the area of the second molar [1]
-
Dehiscence to the second molar [7]
-
Hypersensitivity in the area of the distally exposed root surface of the second molar
-
Alveolar osteitis and soft tissue abscess are severe complications
2.3 Triangular flap design and modification (buccally based triangular flap)
This technique was described by Szmyd [6]. The incision is conducted from the mandibular ramus to the distobuccal crown edge of the second molar, followed by a perpendicular incision obliquely into the mandibular vestibulum, with a length of about 10 mm. In contrast, the modified incision extends over the mucogingival borderline, and the periodontium of the second molar is only touched at the dentofacial edge (Figures 2 and 3). The flap is lingually based on the triangular flap [8].
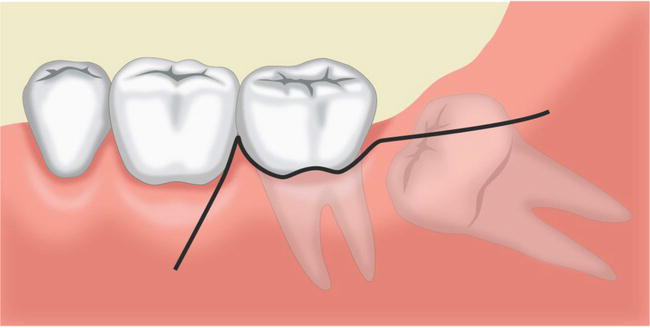
Figure 2.
Triangular flap for the removal of the third molar.

Figure 3.
Modified triangular flap for removal of the third molar.
For suturing, the same suturing technique is used distally (envelop), whereas the perpendicular incision is only adapted with a single coronally placed suture. The main aim is exact repositioning of the gingival margin in the area of the second molar. The loose adaption in the apical portion allows easy relief of a hematoma.
Advantages
-
Reduces the incidence of wound dehiscence
-
A suitable choice for compromised cases of nicotine exposure
-
This flap can be easily moved to the lingual, ensuring a wound closure that is almost tension-free [8]
Limitations
-
Swelling and trismus
-
Pain
-
No significant difference in postoperative complications between the lingually based triangular flap and the traditional buccally based triangular flap after surgery of the third molar [8]
Advertisement
3. Flap techniques for canine exposure or removal
3.1 Background
Canines are among the most commonly impacted teeth after the third molar teeth. Different causes have been suggested and investigated in literature [9]. The impacted canines need to be either exposed or removed to avoid some possible complications. Untreated canines may cause tooth malalignment, root resorption of adjacent teeth, infections, and cystic changes.
The location of an impacted canine will determine the access for surgical exposure or removal. About one-third of the impacted maxillary canines are positioned labially or within the alveolus, while two-thirds are located palatally [10]. Kokich [11, 12] suggested that the following four criteria related to tooth position within the alveolar bone housing need to be carefully evaluated before exposing the impacted canine:
-
The first criterion looks at the labial-palatal position of the impacted canine. When there is labial impaction, the treatment of choice is an open technique (gingivectomy or apically positioned flap). While impaction in the mid-alveolus requires an open or closed technique, a palatal impaction is usually treated using a closed technique.
-
The second criterion evaluates the impaction position relative to the mucogingival junction (MGJ) in an apical-coronal dimension. When the majority of the impacted crown is positioned coronal to the MGJ, the gingivectomy open technique can be conducted. If the crown is located at the MGJ level, an apically repositioned flap is used. When the crown is apical to the MGJ, a closed technique is generally utilized.
-
The third criterion involves the evaluation of the amount of keratinized gingiva (KG) mainly with facial impactions. When there is an abundance of KG, the impacted canine is positioned relatively close to the MGJ, and a gingivectomy procedure is recommended. However, if there is inadequate KG, an apically repositioned flap or closed technique is suggested.
-
The fourth criterion evaluates the mesial-distal position of the canine relative to the lateral incisor. If the canine crown is positioned distal to the mesial aspect of the lateral incisor, an open technique is performed. If the crown is positioned mesial to the lateral incisor, a closed technique for the pataltal eruption of canine.
3.2 Labially impacted canine techniques
Labial canine impaction is usually difficult to approach because aesthetic outcomes of final soft-tissue healing are a challenge. An inappropriate surgical technique or flap design may lead to compromised aesthetic results [12]. During the process of uncovering a labially impacted maxillary canine, mucogingival problems, such as an immersed clinical crown, limited keratinized gingiva, gingival recession, and scarring, may occur if an inappropriate surgical intervention is employed [13]. In addition, the vertical and horizontal locations of the impacted canine also greatly affect orthodontic tooth movements and soft-tissue responses. Therefore, it is critical to make the right decision about the choice of a proper surgical technique to expose labially impacted teeth.
The proposed flap techniques include the window excision of the soft tissue (Figure 4), apically positioned flap, closed eruption technique, and sequential approach.
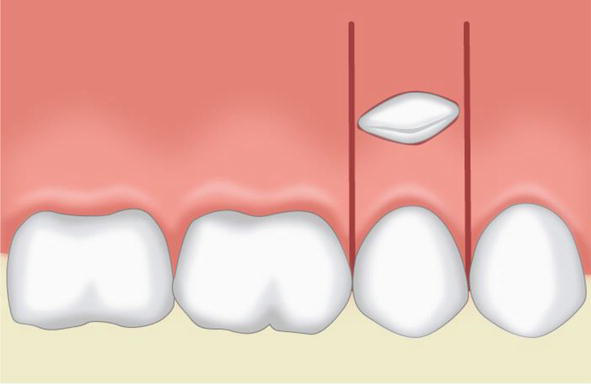
Figure 4.
Window excision at the labial soft tissue opposite to the crown of the impacted upper canine.
3.3 Window excision of the soft tissue
Figure 4 shows the window excision of the soft tissue when the canine crown is coronal to the mucogingival junction.
Advantages
-
Directly expose the crown part
-
Easy to perform
Limitations
-
Sacrifice the gingival tissue
-
Require wider attached gingiva
3.4 Apically positioned flap
Figures 5 and 6 show the apically positioned flap if there is insufficient attached gingiva.
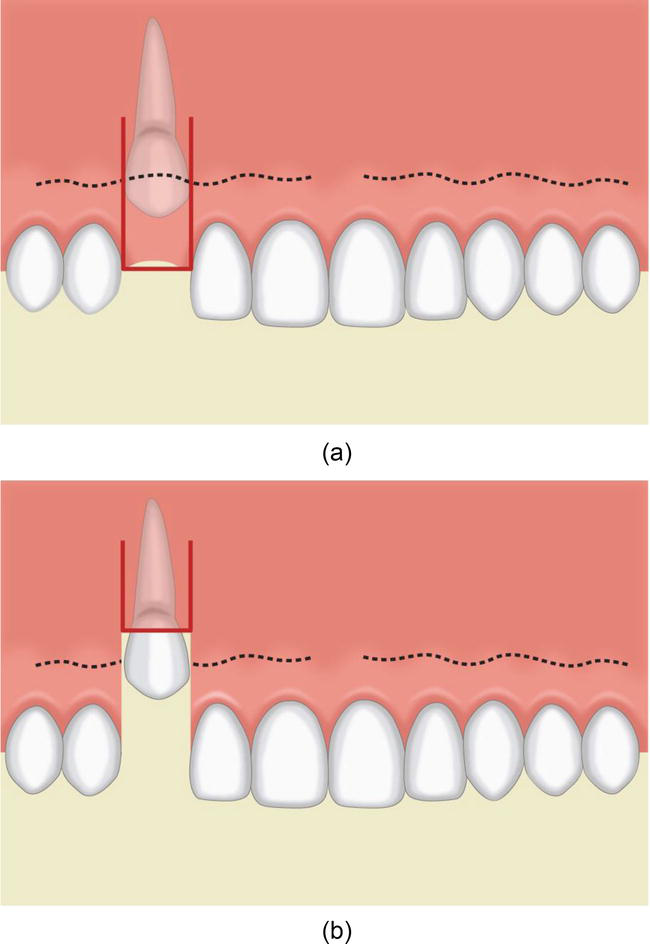
Figure 5.
An apically repositioned flap: (a) outline of the flap; (b) flap repositioned apically to provide a collar of the attached gingiva around the exposed tooth.

Figure 6.
Window is created (top image) labially opposite to the crown of the impacted canine, and (bottom image) the attached free gingival margin is placed apically.
Advantage
-
Preserve attached gingiva
Limitation
-
Not suitable in highly impacted canine
3.5 Closed eruption technique
Figure 7 shows that highly impacted canine and the crown tip are properly aligned mesiodistally.

Figure 7.
Gingival margin flap with bracket and chain bond it to the crown of the impacted canine.
Advantage
-
The closed mucosal flap is more comfortable for patients
Limitation
-
Uncontrollable orthodontic forces on the nonvisible tooth during orthodontic extrusion
3.6 A sequential approach
If a maxillary canine is highly impacted, its crown protrudes labially, or its cusp tip is displaced mesially (Figure 8), two-stage approaches may be indicated, in which exposure is carried out first (Figure 6) and mucogingival surgery such as gingivoplasty is performed at a later stage. Laterally sliding flap (Figure 9) provides additional keratinized tissue with natural color and consistency at the recipient site if adequate keratinized gingival is available over lateral incisor. Pedicle flap can be the second option and can be dissected from both the central and lateral incisor areas to transfer to cover the recipient bed (Figure 9).

Figure 8.
Mesially exposed impacted canine that may require two-stage surgery to achieve minimal attached gingiva.

Figure 9.
The principle of lateral pedicle repositioned flap. R, recipient tooth; D, donor tooth; F, flap; S, split-thickness dissection.
Advantage
-
Achieve 3–4 mm keratinized gingiva in highly impacted canine [9]
Limitations
-
Two-stage surgery
-
Donor site morbidity is expected
Advertisement
4. Periodontal flap surgery
4.1 Background
The main objective of periodontal flap surgery is to eliminate and reduce the pocket depth that cannot be treated conservatively (evidence of bleeding, loss of attachment, or suppuration) with conventional periodontics treatment. Raising surgical flap facilitates removal of the inflamed tissue inside the pocket, provides access for tooth surface cleaning, and helps remove harmful plaque and calculus.
Indications
-
Provide access to the tooth's root surface for instrumentation
-
Correction of gingival overgrowth by gingivectomy
-
Create new periodontal attachment
-
Improve aesthetics and function following gingival recession by the root coverage technique
Contra-indications
-
Poor plaque control
-
Uncontrolled systemic disease
-
Heavy smokers
-
Teeth with poor long-term prognosis
4.2 Full-thickness periodontal flap
Raising full mucoperiosteum exposes the underlying bone. The modified Widman flap [14] is one example of this type of flap. It includes a scalloped incision 1 mm from the crevicular margin involving the interproximal area of the teeth, allowing the flap to be raised without releasing incision (Figure 10).
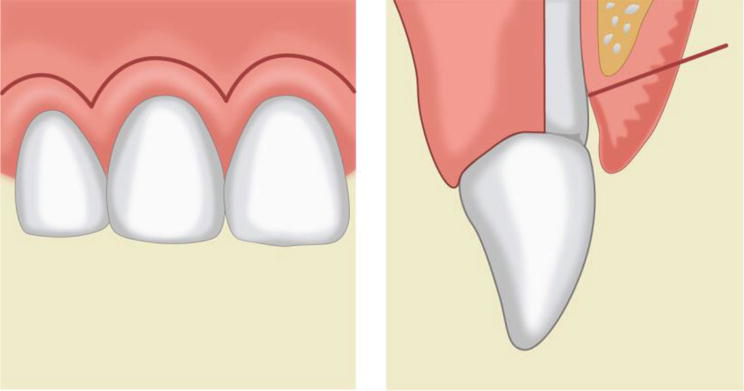
Figure 10.
Modified Widman flap technique. The image is adapted from The Hungarian higher education in dentistry in Hungarian, German, and English.
Advantages
-
Allow close adaptation of soft tissues to the root surface with minimal trauma
-
Less postoperative teeth sensitivity
-
Better aesthetic results
-
Allow root surface debridement
-
The pocket reduction is achieved by long junctional epithelial attachment to the root surface
Limitations
-
Not indicated if osseous surgery is planned
-
Cannot be used for full pocket removal
4.3 The apically repositioned flap
Reverse bevel incision is made at the attached gingiva angled to excise the periodontal pocket in a scalloped fashion. Two releasing incisions are made mesial and distal to the defect. After the flap is elevated, pocketing tissues are discarded, osseous surgery can be performed, and the flap is then apically repositioned and sutured in position as illustrated above in the canine exposure section (Figure 11).

Figure 11.
Apically repositioned flap for periodontal surgery. (a) The bevel, scalloped incision for pocket elimination. (b) The flap positioned apically.
Advantages
-
Expose the alveolar bone and allow osseous surgery to correct infrabony defects
-
Allow excellent access to the root surface for debridement
Limitation
-
Not applicable in the palatal tissue
4.4 Gingivectomy
Beveled incision excises the supra-gingival pocket and allows for gingival re-contouring.
Advantages
-
Suitable for gingival hypertrophy (supra-alveolar pocket)
-
Re-contouring severely damaged gingival tissues
-
Crown lengthening (Figure 12)

Figure 12.
The stages for crown lengthening. (A) Internal beveling; (B) sulcular incision; (C) removal of excess tissues to expose the crown or the gingival overgrowth.
Limitations
-
Not indicated in case of deep "true" infrabony pocket
-
Not suitable for removal of intrabone lesions
-
Row wound exposes the root surface, making it sensitive and susceptible to caries
-
Because of the loss of the attached gingiva, some bone remodeling may occur
Advertisement
5. Mucogingival graft surgery
5.1 Background
Mucogingival graft surgery aims at the correction of local gingival defects. It will be conducted if changing the morphology of gingival margin improves the plaque control, high frenal attachment, and severe gingival recession.
5.2 Split thickness flap
Raising partial soft tissues and leaving the mucoperiosteum attached to the bone are commonly used techniques to address such mucogingival problems. Moreover, pedicle flap includes either laterally, coronally, or double papilla repositioned flaps. The flaps are indicated in very narrow areas of isolated gingival recession or even in the presence of wide recession with adequate door tissues on either side [15].
5.3 Laterally repositioned flap
Two horizontal incisions are made on both mesial and distal sides of defects 1 mm away from the gingival margin of the adjacent tooth. Two vertical incisions are then made perpendicular to the initial incisions on either side, which extend into the alveolar mucosa. Partial-thickness pedicles are reflected on either side of the recession area (Figure 9). The reflection is carried out to a level that would permit free movements of the mesial and distal pedicle flaps. Both pedicles are rotated over the defect to make sure they would remain over the defect without any tension. Subsequently, both pedicles are sutured with 6-0 polypropylene sutures.
Advantages
-
Minimal exposure of the underlying periosteum at the interdental donor sites
-
Rapid wound healing at the donor site
Limitations
-
Cannot be used in a generalized recession
-
Cannot be used if there is an inadequate amount of keratinized tissues at donor sites
5.4 Coronally repositioned flap
A partial-thickness flap is raised around the defect with the help of two horizontal and two vertical incisions on either side of the defect without involving the marginal gingiva of adjacent teeth. To facilitate a tension-free coronal displacement, its base can be separated from the periosteum with the help of a periosteal releasing incision. The flap is then advanced coronally and sutured at the level of cementoenamel junction (CEJ) using 5-0 polypropylene sutures (Figures 13 and 14).

Figure 13.
Coronally repositioned flap used to cover localized recession. The top image shows the recession area, and the incision line is done 4–5 mm from the gingival margin; the bottom image shows that partial-thickness flap is raised and sutured coronally.

Figure 14.
Free gingival graft is applied to cover the root surface with less amount of attached gingiva.
5.5 Free gingival grafts
This graft is a harvested tissue and is completely removed from the blood donor area, and it is used to augment the amount of the attached (keratinized) gingiva. This approach can be only used with the combination with another surgical approach.
5.6 Two-stage surgical techniques
Two-stage surgical techniques use double pedicle flap with a connective tissue graft, followed by coronally advanced flap.
Advantages
-
Treatment for a severe localized gingival recession
-
Excellent color matching and dual blood supply to graft
-
Very predictable results
-
Can be used if minimal keratinized tissue is present
Limitations
-
Requires good pedicel length
-
Two-stage surgery
-
A free graft is required
Advertisement
6. Flap for dental implant bed preparation
6.1 Background
Two-stage flap techniques are commonly used for dental implant surgery and include a flapless (e.g., Punch or Half Punch) flap and full-thickness flap, such as mid-crest, double papilla preservation flap. Full-thickness flap might be more suitable for immediate implantation; the flapless flap is superior to full-thickness flap in cases of less inflammation and less morbidity, has shallower biological width, and shows better aesthetic results [16].
6.2 Punch flap
A small hole in the keratinized mucosa is required to be present on the crest of the ridge at the area of interest (Figure 14). This punch can be created using a blade or punch drill. Precise placement of the cut can be obtained using the surgical guide with the help of the planning software (Figure 15).

Figure 15.
Punch flap (flapless) at mid-crest of ridge.
Advantages
-
Minimal surgery
-
Minimal postoperative pain/discomfort
-
Suitable for one-stage surgery
Limitations
-
Simultaneous bone grafting is not possible
-
Minimal exposure to the bone for thickness evaluation
-
Require sufficient keratinized mucosa
6.3 Half punch
In the case of the presence of inadequate or deficient buccal tissues, half punch approach is used. Half punch flap is conducted with horizontal crestal incision and reflects full-thickness flap buccally. Subsequently, punch approach is used lingually or palatally to remove minimally required tissues for implant placement (Figure 16).

Figure 16.
Half punch flap used for implant bed preparation.
Advantage
-
One-stage implant surgery with possible simultaneous bone grafting
6.4 Mid-crestal incision
Mid-crestal incision is performed at the middle of the ridge bone, and buccal and lingual/or palatal flaps are then raised to expose the full surgical site (Figure 17).

Figure 17.
The edentulous ridge with minimal attached gingiva. Half punch flap is performed.
Advantages
-
This flap can be used for both one- and two-stage implant surgery
-
Buccal and palatal/lingual bone grafting is possible
Limitation
-
Requires sufficient buccal and palatal tissues
6.5 Palatal/lingual crestal flap
The incision is similar to mid-crestal incision; however, it is made more toward the palatal side/lingual. The flap is then raised to perform the bone preparation (Figure 18).

Figure 18.
Mid-crestal incision used during implant bed preparation.
Advantages
-
Suitable in cases when there are less buccal tissues available to raise full-thickness flap
-
Bone grafting can be performed buccally or palatally/lingually
-
Suitable for both one- and two-stage implant surgery
6.6 Mesial papilla preservation flap
This flap is designed to maintain the interdental papilla for aesthetics in some cases.
In this flap, vertical releasing incision distal to the papilla is made and is connected to a crestal incision on the other side of the defect. An intrasulcular incision on the distal tooth is performed, and the flap is raised, followed by implant bed preparation (Figure 19).

Figure 19.
Platatal crestal flap used for implant bed preparation.
Advantages
-
Good aesthetic results
-
Minimal surgery and soft tissue manipulation
Limitations
-
Not suitable if bone grafting is required
-
Used for the second stage of implant surgery to help get maximum aesthetic results by preserving the papilla
6.7 Distal papilla preservation
This flap is opposite to mesial preservation flap, and the aim is to preserve the distal side of the defect to allow bone grafting (Figures 20 and 21).

Figure 20.
Mesially papilla preserved incision for implant bed preparation.

Figure 21.
Double papilla preservation with two vertical releasing incisions.
6.8 Double papilla preservation
This flap is designed to preserve both mesial and distal papilla at the defect area. Two vertical incisions are performed and connected with lingual or palatal crestal incision, thus allowing the release of the mucoperiosteal flap toward the buccal aspect.
Advantages
-
More aesthetic results
-
Suitable for the second stage of implant surgery where the mobilization of a good amount of tissues may be required
Limitation
-
Vascularity may be compromised in the narrow space
6.9 Full-thickness flap reflection for large edentulous spaces (book flap)
The buccal or lingual mucoperiosteal flap can be reflected, allowing an alveolar split to be done using thin osteotomes for alveolar ridge expansion if required.
Advantages
-
Wide exposure allows observing the undercut lingually or buccally
-
Easy to lean and perform alveoloplasty
-
Easy to perform bone cutting and splitting
Limitations
-
Bone devitalization and subsequent remodeling resorption in narrow ridge [17].
-
Less predictable outcomes
6.10 Partial-thickness flaps for ridge expansion
This is a minimally exposed osteoperiosteal flap to overcome the limitation of full-thickness flap for the wide edentulous area when the resulting vascularity may jeopardize the outcomes (Figure 22).

Figure 22.
Full ridge exposure using the full thickness flap buccally and lingually.
Advantages
-
Maintain the integrity of periosteum
-
Maintain bone vitality (vascularity)
-
Alveolar width stability, that is, minimal postoperative resorption compared with full-thickness flap
Limitations
-
The bone is cut blindly; therefore, the surgeon must have a good conceptualization of the alveolar anatomy to not miss the midpoint of the alveolus. The surgeon should avoid extending to the vestibular depth or palatally directed osteotomy
-
Requires extensive flap dissection [17]
Advertisement
7. Endodontic surgery flap
7.1 Background
Flap design in periapical surgery should be adequate for the planned surgical procedure, offering good access to the zone surrounding the affected apexes without altering the soft-tissue circulation. The flap should be a firm continuous incision and not cross an underlying bony defect. If a vertical incision is needed, it should be in the concavities between bone eminences. The vertical incision should not extend into the mesiobuccal fold, and its termination of the gingival crest must be at the mesial or distal line angle of the tooth. Additionally, the base of the flap must be at least equal to the width of its free end. The most frequently used flap in periapical surgery is the Luebke-Ochsenbein flap involving submarginal incision, with semilunar or Partsch flap variants.
7.2 Luebke-Ochsenbein flap
A horizontal incision is made in the attached gingival tissue about 3–4 mm above the gingival margin, with two vertical releasing incisions on either side of the flap located one or two teeth distal to where the lesion is located (Figure 23).

Figure 23.
Partial-thickness flap before ridge expansion for future dental implant insertion.
Advantages
-
This type of flap is easy to detach
-
It is less aggressive with the gingival tissue than an intrasulcular incision flap
-
It is useful in patients with fixed prosthesis restorations because of less recession of the gingival margin and interdental papillae [17, 18, 19]
Limitation
-
It can leave a postsurgical scar if the repositioning sutures are not performed adequately [20]
7.3 Partsch flap
The semilunar (Partsch) flap is a variant involving a submarginal incision in the alveolar mucosa to form a crescent- or semilunar-shaped flap (Figure 24). The semilunar flap is almost exclusively used for the maxillary canines [21]. Care is required to avoid performing the incision above the bone defect.

Figure 24.
Submarginal incision and two vertical incisions mesial and distal to the defect area.
Advantage
-
Small incision suitable for upper canine surgery
Limitations
-
Limited surgical access to the root apex
-
Flap tension is high due to the presence of muscle fibers, making suturing difficult and increasing the risk of suture dehiscence [5, 22]
7.4 Neumann flap
This flap involves intrasulcular incision in its triangular and trapezoidal versions and offers perfect access for periapical surgery, with sufficient access to the affected bone and lesion-related roots. The intrasulcular incision may be triangular or trapezoidal (Figure 25). The most common intrasulcular flap involves a triangular incision with a single vertical releasing incision located one or two teeth distal to the lesion (Figure 26). This flap is characterized by increased tension, and the traction forces increase especially at the fixed extremity. This technique allows for easy flap repositioning after periapical surgery.

Figure 25.
Luebke-Ochsenbein flap is used clinically for periapical surgery.

Figure 26.
Semilunar flap in a form of crescent.
Advantage
-
This technique allows easy flap repositioning after periapical surgery
Limitation
-
Increased tension and traction forces
7.5 Papilla base incision flap
This flap, which was originally described by Velvart, is characterized by a horizontal incision following the dental sulcus along the neck of the teeth and extending to the base of the papillae (Figure 27). The papillae adhere for posterior suturing of the flap. A vertical releasing incision is made to maximize the exposure.

Figure 27.
Clinical application of Partsch flap for periapical surgery.
Advantage
-
Produces less recession at the interdental papillary level than a sulcular incision [23]
Limitations
-
A surgically complicated flap requiring adequate surgeon experiences
-
Requires the presence of enough healthy attached gingiva for suturing
7.6 Papilla-preserving flap
A horizontal incision is made following the dental sulcus to the dental papilla, and the vertical releasing incision is seated away from the papilla (Figures 28–33) [19].

Figure 28.
Trapezoidal flap with two releasing incisions.

Figure 29.
Triangular flap with a single releasing incision.

Figure 30.
Clinical application for the intrasulcular trapezoidal flap.

Figure 31.
The papilla adhered to the bone and the raised full mucoperiosteal flap.

Figure 32.
The raised papilla preservation mucoperiosteal flap.

Figure 33.
The raised palatal full mucoperiosteal flap for palatal periapical surgery.
Advantage
-
This flap is useful in teeth with a generous mesiodistal width, affording an adequate surgical field
Limitations
-
The narrow neck needs careful releasing, careful adaptation, and suturing
-
This flap may be not suitable in narrow mesiodistal distance between teeth
7.7 Palatal flap
A festoon flap is performed at the gingival margins on the palatal side. This flap is used in periapical surgery of the palatal roots of the maxillary molars. Palatal releasing incisions are not necessary. If any such incisions are made, they should be performed between the canine and premolar, representing the vascularization limit between the nasopalatine artery and the anterior palatine artery, or distal to the second molar behind the emergence point of the anterior palatine artery [24].
Advantage
-
Useful in cases in which the palatal roots of molars or lateral incisors require exposure
Limitations
-
If the flap needs to be expanded to gain greater visibility, the incision can be extended mesially to the canine
-
This flap may cause pain and discomfort for the patient postoperatively
-
Chance of hematoma formation may jeopardize the blood supply of the flap
Advertisement
8. Flaps for management of oroantral communication
8.1 Background
Oroantral communication/fistula is an unnatural communication between the oral cavity and the maxillary sinus. These complications occur most commonly during the extraction of upper molar and premolar teeth (48%). The major reason is the anatomic proximity or projection of the roots within the maxillary sinus [25]. Other causes of oroantral communication/fistula include tuberosity fracture, dentoalveolar/periapical infections of molars, implant dislodgement, maxillary sinus, trauma (7.5%), presence of maxillary cysts or tumors (18.5%), osteoradionecrosis, flap necrosis, and dehiscence following implant failure [25, 26]. Two basic principles must be considered while operating for Oroantral communication/fistula. First, the sinus must be free of any types of infection with adequate nasal drainage. Second, closure must be tension-free and consists of broadly based, well-vascularized soft tissue flaps over the intact bone. Successful closure of the oroantral fistula should be preceded by the complete elimination of any sinus pathology, the fistulous tract, sinus infection, degenerated mucosa, and diseased bone [27].
The most common flap procedures may be categorized into local flaps, distant flaps, and grafting. The flaps involving rotating or advancing soft tissues include buccal flap, palatal flap, submucosal tissue flap, and buccal fat pad and tongue flap [26]. The procedures utilizing buccal mucoperiosteal flap for closure include straight-advancement flap, rotation-advancement flap, transverse flap, and sliding flap techniques, and those utilizing palatal mucoperiosteum include straight-advancement flap, rotational advancement flap, hinged flap, and island flap procedures [26]. Double-layer closure utilizing local tissues includes the combination of inversion and rotational advancement flaps, double overlapping hinged flaps, double island flaps, and superimposition of reverse palatal and buccal flaps. However, the studies over the last 50 years point out the lack of consensus for a uniformly successful procedure [28].
Here we illustrate the most common flaps used for closure of oroantral communication/fistula: the buccal flap and the palatal pedicle flap techniques.
8.2 Buccal advancement flap
It has been described [14, 29] the use of a buccal flap with a thin layer of buccinator muscle to close an oroantral defect. Later, [30] reported a buccal sliding flap technique, which is still in use, as a tool to close small to medium size (<1 cm) lateral or mid-alveolar fistulas, located either laterally or in the middle of the alveolar process. Krompotie and Bagatin [13] reported the immediate closure of an oroantral communication by a rotating gingiva-vestibular flap. This technique can also be employed for closing oroantral fistulas. It is a modification of a vestibular flap in order to avoid lowering of the vestibular sulcus, an event that takes place normally when using vestibular flaps. Two vertical release incisions are made to provide a flap with dimensions suitable for closure of the antral communication (Figure 34).

Figure 34.
The buccal advancement flap is used to close OAC (arrow).
Incision removal of the epithelial lining of the palatal mucosa behind the communication might also be required. The flap with a trapezoidal shape consists of both epithelium and connective tissues and is positioned over the defect using mattress sutures from the buccal flap to the palatal mucosa.
Advantage
-
It is possibly utilized in cases of severly resorbed alvealr ridge, and the fistula is located in a more mesial area [31]
Limitation
-
Loss of vestibular depth buccally
8.3 Palatal pedicle flap technique
The first procedure for closing oroantral fistulas using a palatal full-thickness flap was described by Ashley [26, 32]. After excising the epithelium from its edges and cutting the palatal fibro-mucosa, the flap is created with an axial stack with a posterior base, supplied by the greater palatine artery. The palatal flap with its total thickness laterally rotated must have a large base to include the greater palatine artery at the site of its exit from the foramen (Figure 35) [33, 34]. The anterior extension of the flap must exceed the diameter of the bony defect and have a length sufficient to allow its lateral rotation and replacement, and the suture has no exerting tension on the vestibular mucosa [35]. Further improvement of the techniques was advocated [35, 36] by adding a flap of mucosa to the connective tissue island to cover the raw area of the palatal bone. The bone is covered, and the island flap retains excellent mobility without causing bunching of the mucosa of the hard palate and recipient site.

Figure 35.
The palatal rotation flap used to close OAC (arrow).
Advantages
-
Good vascularization, adequate thickness, and optimal tissue quality
-
The use of mucous membrane from the hard palate. In 1980, Ehrl demonstrated the possibility of employing this technique with wide fistulas 1 cm in diameter [37]
-
This method allows replacement of the denture a short time after the wound healing
Limitation
-
It is only indicated if the fistula is located at the area of the premolar to avoid excessive rotation of the flap
-
The area of the palatal flap will heal by secondary epithelialization, which causes pain and discomfort
-
Necrosis of the flap can happen if excessive rotation to the flap is performed
8.4 Buccal pad of flat flap (BPF)
Since Egyedi reported the BFP flap as a suitable method to close the OAC, oronasal communication, and maxillary postsurgery defects, the technique has been widely used. In addition, according to the study by Rapidis et al. [38], the BFP can be used as a free flap to close oral defects. Tideman et al. described the detailed anatomy, vascularization, and operative techniques of BFP [39]. The pedunculated BFP has been employed for the reconstruction of an oral defect of moderate size following surgical removal of a malignant lesion [38]. A gentle dissection with fine curved artery forceps exposes the yellowish-colored buccal fat. The buccal fat pad flap, especially the pedicled type, has been used most commonly for the closure of the OAF due to the location of the buccal fat pad, which is anatomically favorable, and due to the easy and minimal dissection, with which it can be harvested and mobilized.
Advantages
-
Good rate of epithelialization [40]
-
Low rate of failure [40]
Limitations
-
Mild reduction in the vestibular height
-
A second surgery is required in order to achieve closure if there is a low rate of recurrence of fistulas
8.5 Double-layer closure techniques
8.5.1 Palatal inversion flap and buccal advancement flap
This technique designs the palatal inversion flap on the basis of the greater palatine vessels after measuring the bone defect, but not the soft-tissue defect, as shown in Figure 35. Once the flap is raised, the residual palatal raw surface is left to heal by secondary intension with the formation of the granulation tissue. The horizontal palatal flap is then inverted so that the oral palatal epithelial surface covers the bone defect and faces the maxillary sinus. Subsequently, it will be covered by the buccal advancement flap that is released by extending the incision inside the cheek from the gingivolabial sulcus to have a wide base and ensure a good blood supply, as shown in Figure 34.
Advantages
-
Indicated if there is an increased risk of wound breakdown and recuurant oroantrual defect
-
It provides epithelial covering to both the superior and inferior surfaces
-
Blood perfusion of the palatal flap is better than that of the single technique
Limitations
-
It has a risk of subsequent pathology
-
Perfusion of buccal flaps is poor
-
Narrowing of the gingivobuccal sulcus may occur
8.5.2 Closure of oroantral fistula using a buccal fat pad (BFP)
BFP is anatomically favorable, and the easy and minimal dissection of the fat tissue from the buccal pad of fat and then harvesting and mobilization made it a popular technique (Figure 36). Furthermore, it has excellent blood supply. A quick surgical technique is preferred due to fact that BFP and the defects to be covered are located in the same surgical field, and a good rate of epithelialization allows for replacement of the mucoperiosteal flap without loss of vestibular depth.

Figure 36.
Intraoral photograph shows the harvested buccal fat and is adapted to the defect in the molar and premolar/molar areas.
Advantages
-
Low rate of complications
-
Minimal donor site morbidity
-
Easy and versatile technique
-
No loss of vestibular depth
Limitations
-
While harvesting BFP, perforation or/and shrinkage may occur
-
The amount of BFP is inadequate in some cases
8.5.3 Double-layer closure techniques
This technique combines BFP and buccal advancement or skin flaps. BFP can be covered by the partial thickness skin flap [41] or buccal advancement flap, especially for defects larger than 5 × 1 cm2. This technique can also be better managed with the use of BFP with buccal advancement flap than BFP alone [42] (Figure 37).

Figure 37.
Illustration shows harvesting BFP from the buccal tissue, and the buccal advancement flap is then sutured.
Advantages
-
Provides more stability
-
Can be used when there is a deficient BFP for closure
-
Can be used in cases where a trapezoidal flap is raised for some reasons and in cases with perforation and shrinkage of BFP [43, 44, 45]
-
Used to minimize the risk of shallow sulcus [42]
Limitations
-
More time is needed to perform the surgery
-
An experienced surgeon may be needed
-
It requires high patient's compliance
Advertisement
9. Conclusions
A wide variety of intraoral flaps and their modifications have been reported in the literature. This chapter illustrates some familiar flap techniques, as well as their advantages and limitations. The application and design of each flap should be tailored to the patient's diagnosis and needs. Surgeons should be aware of patient diagnosis, the anatomical limitation, and the application of different flap's designs. Careful planning, implications, and selection of suitable flap designs would affect final aesthetic outcomes or postoperative morbidity, which may have important medical-legal and economic impacts.
Advertisement
Conflict of interest
The authors declare no conflict of interest.
© 2020 The Author(s). Licensee IntechOpen. This chapter is distributed under the terms of the Creative Commons Attribution 3.0 License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
How to cite and reference
chapter statistics
1788 total chapter downloads
1 Crossref citations
More statistics for editors and authors
Login to your personal dashboard for more detailed statistics on your publications.
Access personal reporting
Related Content
This Book
Next chapter
Interdental Brushes in Maintaining Periodontal Health
By Esra Guzeldemir-Akcakanat
Related Book
First chapter
Introductory Chapter: Saliva - The Future of Disease Diagnostics
By Gokul Sridharan
We are IntechOpen, the world's leading publisher of Open Access books. Built by scientists, for scientists. Our readership spans scientists, professors, researchers, librarians, and students, as well as business professionals. We share our knowledge and peer-reveiwed research papers with libraries, scientific and engineering societies, and also work with corporate R&D departments and government entities.
More About Us
double flap design envelope video
Source: https://www.intechopen.com/chapters/71271
Posted by: thompsonwhirds.blogspot.com
0 Response to "double flap design envelope video"
Post a Comment